Two Tracks, One Athlete: Return-to-School vs Return-to-Sport Staging
I expected one recovery timeline—I found two vocabularies (RTS means school in one protocol and sport in Berlin) and clocks that do not compare. This piece maps parallel return-to-learn and return-to-sport checklists and where aerobic prescription must follow the school leg.
Caution
Not medical advice. Educational use only. Data from published literature.
Pulling return-to-learn and return-to-sport checklists side by side, I expected one timeline. I found two vocabularies—RTS means school in one Canadian protocol and sport in Berlin—two median clocks (35 vs 38 days in one youth cohort), and chart data saying we still release both tracks too early, often on different schedules PMID: 31396150 PMID: 24925965.
This is a methods piece, not a replacement for CISG appendices or your district’s return-to-play law. It maps two parallel staging checklists (RTL and RTP), shows where they attach to intensity bands (%HR, RPE, symptom cap) and weekly volume (minutes × days), and flags when published recovery numbers cannot be compared. Athletic trainers and school staff will find the most actionable material in Section 4 and the dual-track SOP; researchers and trainees will find the endpoint and chart-review critique in Section 3—skippable on first read if you only need staging labels for tomorrow’s clinic.
Setting a sub-symptom heart-rate band and negotiating weekly minutes both assume the staging question is mostly settled: once symptoms allow, you advance. In clinic, the adolescent often carries two advance rules at once—what the school will permit and what the sport program will permit—and those rules are not written in the same document.
1. Two checklists, one student
Sport-related concussion management now routinely describes graduated return-to-learn (RTL) and graduated return-to-sport (RTP) as parallel processes. Berlin 2017 was the first International Conference on Concussion in Sport (CISG) consensus to publish paired strategies: a four-step return-to-school progression and a six-step return-to-sport progression in the same statement PMID: 28446457. Amsterdam 2022 retained that skeleton, refined symptom rules (mild and brief exacerbation on a 0–10 scale), and stated explicitly that RTL and RTP may occur in parallel while full RTL should precede unrestricted RTP PMID: 37316210.
The logic sounds coordinated. The operational reality often is not.
A common failure mode: the athlete is cleared for light aerobic work or non-contact drills on the sport track while still on partial school attendance or formal accommodations on the learning track—or the reverse, full days at school while still symptom-limited for sport. Neither is automatically wrong; guidelines allow overlap in early stages. What breaks down is documentation and communication: the school sees one stage label, the trainer another, and the family hears “cleared to exercise” without hearing “not cleared for contact” or “still on reduced screen time.”
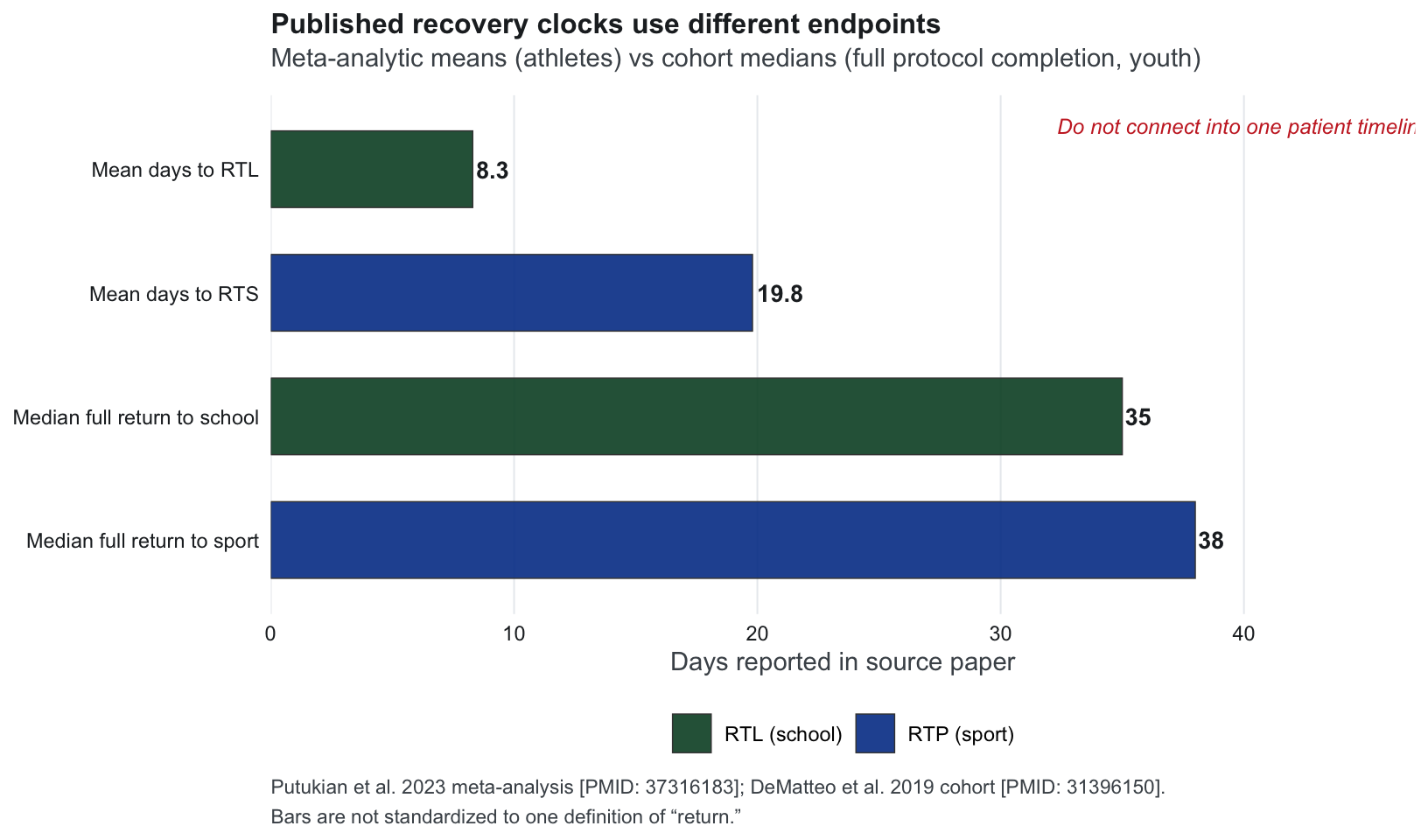
Canadian chart reviews quantify the asymmetry. Carson et al. found 43.5% of concussion cases returned to sport too soon and 44.7% returned to school too soon in a 2006–2011 cohort PMID: 24925965. A follow-up review (2011–2016) showed premature RTP relapse falling (26.7%) while premature RTL relapse remained high (42.6%)—consistent with structured RTP reaching clinics before structured RTL PMID: 35292472. Meta-analytic work in athletes reports mean days to RTL 8.3 versus RTS 19.8, with 93% achieving full RTL by 10 days without new academic support—yet cohort medians for full return in youth can run 35 days (school) and 38 days (sport) when stage-by-stage progression is tracked PMID: 37316183 PMID: 31396150. Those numbers measure different endpoints; comparing them without a shared definition is its own error mode.
For aerobic prescription specifically, the mismatch matters. Heart-rate bands and weekly minutes are usually written on the assumption that cognitive load is negotiable. If the student is still in RTL step 1–3—homework bursts, partial days, screen limits—adding even “sub-symptom” walking or cycling on the sport track can stack physical and cognitive load in the same 24 hours. The limiting track may be school, not the heart-rate formula.
Why the school column is not “soft” sport advice
The sport track dominates conference tables and athletic-trainer workflows. The school track has its own literature—not a footnote to RTP.
Halstead et al.’s AAP guidance on return to learning describes post-concussion classroom difficulty as common and calls for medical-home coordination with schools on environmental and academic adjustments PMID: 24163302. Purcell, Davis, and Gioia’s systematic review on return to school after sport-related concussion reports that 17–73% of students received accommodations or had difficulty with school return—wide heterogeneity, but not a rare edge case PMID: 29500251. Factors in that review include symptom burden, rest timing, age/grade, and course load—variables absent from most aerobic-exercise trial arms.
Canadian primary-care writing on returning to school emphasizes staged re-entry and communication between clinic and classroom—not assuming full attendance on calendar alone PMID: 37315976. REAP-style workflows explicitly bridge remove–educate–adjust–pace communication between emergency, medical, and school stakeholders PMID: 26589561. When this piece asks where aerobic prescription “attaches,” the honest answer is: often on the sport leg in clinic notes, while the evidence for load management is split across both legs.
DeMatteo’s systematic review adds a sobering implementation note: RTA/RTS protocols are widely adopted, yet paediatric efficacy evidence remains thin—supporting 1–2 days of rest then graduated progression, but not proving that any one staging checklist is validated in trial PMID: 32153982. Staging is therefore as much a documentation and coordination problem as a physiology problem.
Abbreviation lock (read before the table)
Different research groups label the same idea differently—not because the field is unusable, but because school and sport tracks were formalized by separate literature streams that merged only recently (Berlin 2017 onward).
| Framework | School / learn track | Sport / activity track |
|---|---|---|
| CISG Berlin & Amsterdam | RTL (return to learn) | RTP / RTS (return to sport) |
| DeMatteo / CanChild protocols | RTS = return to school | RTA = return to activity (play/sport) |
| Canadian chart reviews | RTL | RTP |
This article uses RTL + RTP in prose. When citing DeMatteo, translate once: RTS (DeMatteo) = school. One shared row in your note prevents the collision from reaching families.
2. Four-step RTL vs six-step RTP (CISG)
Table note: Step labels and activities below follow Amsterdam 2022 appendices (current CISG) PMID: 37316210. Berlin 2017 used the same four-step RTL / six-step RTP structure with closely related activity descriptions PMID: 28446457. Both recommend 24–48 hours of relative rest before step 1; Amsterdam allows symptom-limited activity within 24 hours of injury with defined exacerbation limits. Minimum 24 hours per step when advancing without symptom worsening.
Return-to-learn (RTL) — four steps
| Step | Mental activity (aim) | Activity at each step | Goal |
|---|---|---|---|
| 1 | Daily activities without more than mild, brief symptom exacerbation* | Typical day activities (e.g., reading) with minimized screen time; start 5–15 min and increase gradually | Gradual return to typical activities |
| 2 | School activities | Homework, reading, or other cognitive work outside the classroom | Increase tolerance to cognitive work |
| 3 | Return to school part time | Partial school day and/or more rest breaks during the day | Increase academic participation |
| 4 | Return to school full time | Progress until a full day is tolerated without more than mild exacerbation* | Full academic load; catch up on missed work |
* Mild and brief exacerbation (Amsterdam): increase of ≤2 points on a 0–10 symptom scale for <1 hour compared with pre-activity baseline PMID: 37316210.
Return-to-sport (RTP) — six steps
| Step | Exercise strategy | Activity | Goal |
|---|---|---|---|
| 1 | Symptom-limited activity | Daily activities that do not exacerbate symptoms (e.g., walking) | Gradual reintroduction of work/school |
| 2 | Aerobic exercise | 2A—Light (~≤55% age-predicted max HR) then 2B—Moderate (~≤70% max HR): walking or stationary cycling; may add light resistance if symptoms stay mild* | Increase heart rate |
| 3 | Individual sport-specific exercise | Drills away from team; no head-impact risk (medical clearance if inadvertent head impact possible) | Movement, change of direction |
| 4 | Non-contact training drills | High-intensity drills (e.g., passing); may rejoin team environment | Usual exercise intensity, coordination, thinking load |
| 5 | Full-contact practice | Normal training including contact | Confidence; coaching assessment |
| 6 | Return to sport | Normal game play | Unrestricted competition |
Amsterdam gate for steps 4–6: begin only after resolution of symptoms, cognitive abnormalities, and other concussion-related findings including with exertion PMID: 37316210. Berlin gate for children: do not return to sport until successfully returned to school, while early symptom-limited physical activity remains appropriate PMID: 28446457. Davis et al.’s child-management review similarly recommends schools not return to sport until successful return to school, with early symptom-limited activity PMID: 28455361.
Where the tracks meet (coordination rules)
| Source | Parallel tracks? | School-before-contact rule | Evidence strength |
|---|---|---|---|
| Amsterdam 2022 | RTL and RTP may run in parallel | Complete full RTL before unrestricted RTP; youth should reach full-time school before RTP steps 4–6 | Consensus + systematic review PMID: 37316210 |
| Berlin 2017 | Early physical activity while symptomatic | No sport until successful return to school | Consensus PMID: 28446457 |
| DeMatteo 2019 cohort | Stages 1–3 of school (RTS) and activity (RTA) simultaneously | RTA stage 6 (full contact) delayed until full, successful school reintegration (RTS) | Prospective cohort n=139 PMID: 31396150 |
| DeMatteo 2020 SR | Protocols adopted in practice | 1–2 days rest then graduated RTA/RTS (DeMatteo labels); little paediatric efficacy evidence for either protocol | Systematic review PMID: 32153982 |
Reading the overlap: Amsterdam RTP step 1 explicitly reintroduces daily activity—including school-related load—while RTL steps 1–2 still cap screen time and homework tolerance. Sport step 2 is where published %HRmax bands attach: light then moderate aerobic work. That can be allowed on the sport checklist while RTL step 3 (partial school) is still active—precisely the zone where families need both labels on one plan.
3. How to read the recovery numbers (without merging the tracks)
Section 2 lists steps; the literature quantifying those steps uses different rulers. Three statistical habits—none of them exotic—explain most double-counting errors when RTL and RTP data sit in the same conversation.
Three numbers that do not compare
| Number (source) | What it actually measures | Common misread |
|---|---|---|
| Mean ~8.3 d to RTL (athletes; meta-analysis) PMID: 37316183 | Average days until RTL across heterogeneous studies | “Most kids are back to full school in eight days” |
| 93% full RTL by 10 d (same meta-analysis) PMID: 37316183 | Proportion achieving full RTL without new academic support by day 10 | Same as row above—but endpoint is full, not first step |
| Median 35 d (school) / 38 d (sport) (youth cohort; stage tracking) PMID: 31396150 | Full return on DeMatteo school (RTS) and activity (RTA) protocols | “Meta says 8 days; cohort says 35—someone is wrong” |
| 43.5% / 44.7% returned too soon (chart review) PMID: 24925965 | Marginal proportion of all cases judged premature on RTP / RTL | “If we advance sport, 43% relapse” (not supported without a 2×2 table) |
| 26.7% / 42.6% premature with relapse (later chart review) PMID: 35292472 | Marginal counts of cases where premature RTP / RTL and relapse co-occur in chart documentation | Confused with P(relapse | premature) |
Means from meta-analyses, medians from single cohorts, and percentages from chart reviews answer different questions on different endpoints. Collapsing them into one “recovery timeline” is a methods error, not a disagreement among experts.
Figure 1 — Recovery clocks measure different endpoints
Figure 1. Bars visualize four published summary statistics, not one recovery curve. Meta-analytic means describe aggregated study endpoints in athletes; cohort medians describe full protocol completion in one youth sample. Section 3 argues against quoting any single bar as “typical recovery.”
Figure 2 — Sport vs school track in chart reviews (different metrics)
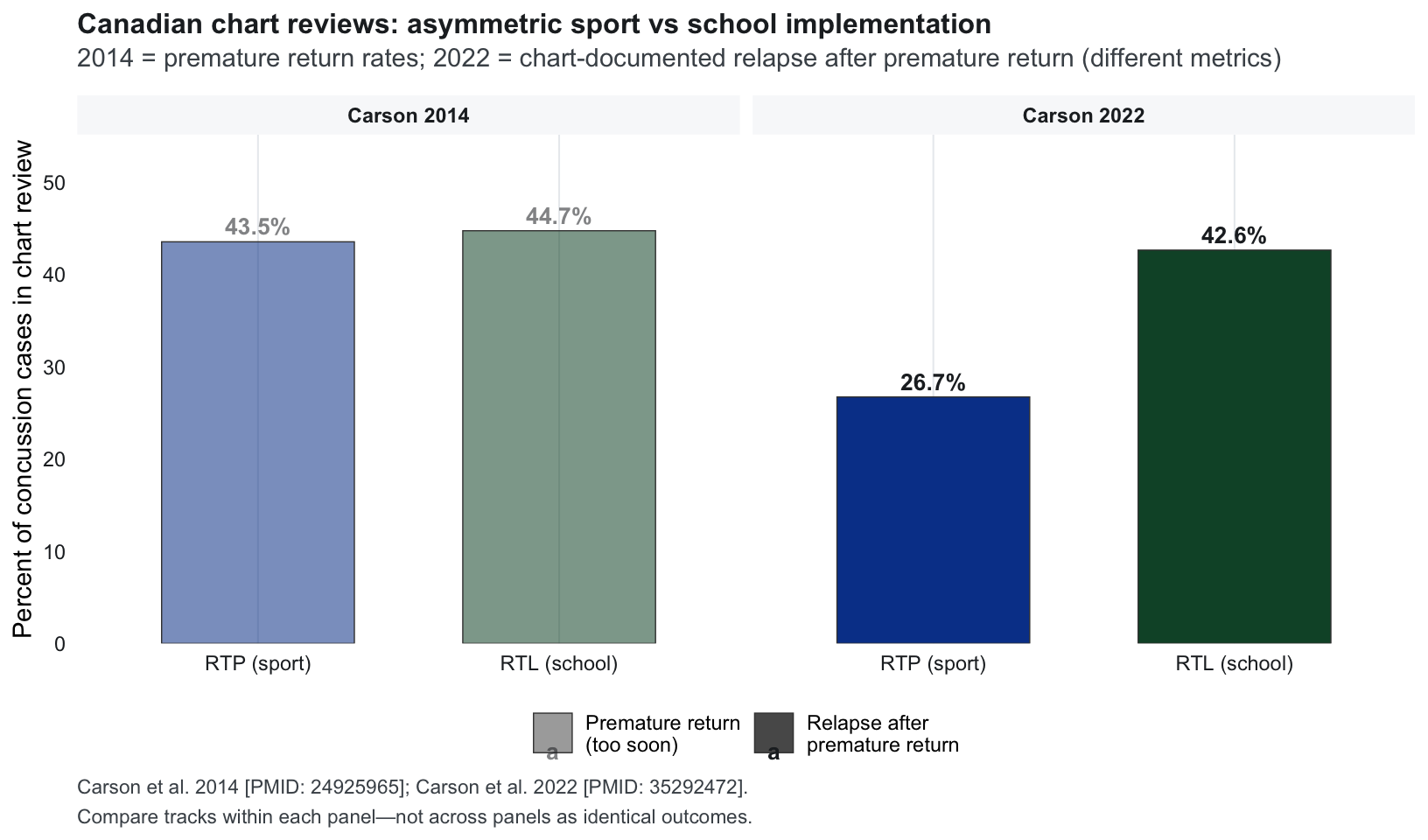
Figure 2. Carson’s two chart reviews use different outcome labels across eras. The pattern worth retaining: school-track problems remain visible even when sport-track premature relapse improves—consistent with RTL tooling lagging RTP in many offices PMID: 35292472.
Marginal vs conditional proportions
Carson-style chart reviews are essential for showing implementation gaps, but their percentages are usually of all concussion cases, not of athletes who were cleared early.
Without published cell counts (premature × relapse), you cannot invert a marginal percentage into a personal risk statement. A defensible clinical read is associative: premature advance on either track still appears common, and relapse after premature advance still appears in charts PMID: 24925965 PMID: 35292472—not that a specific RTL step confers a known relapse probability.
Mean, median, and heavy tails
Recovery days are typically right-skewed: most adolescents recover within weeks; a minority extend much longer. Means (meta-analysis) and medians (DeMatteo cohort) can both be correct yet far apart if long tails pull means or if cohorts define “return” differently.
Putukian et al. also report I² ≈ 99% for days-to-RTL and days-to-RTS outcomes PMID: 37316183—meaning study definitions and populations differ enormously. Figure 1 shows why a single “days to return” number misleads: wide confidence intervals on a meta-analytic mean describe uncertainty about the average across studies, not the spread for the next patient. Individual clocks will often sit outside any single quoted band.
Dual-track state is a cross-classification—not a single stage label
An athlete at RTL step 3 (partial school) and RTP step 2B (moderate aerobic) occupies one cell in a 4×6 grid, not “step 3 overall.” Guidelines permit some combinations; Amsterdam restricts RTP steps 4–6 until symptom resolution with exertion and expects full-time school before those high-risk sport stages PMID: 37316210.
| RTL (school) | RTP (sport) zone | Guideline read |
|---|---|---|
| 1–2 (home / homework) | 1 (symptom-limited daily activity) | Overlap expected; cap total cognitive + physical load same day |
| 3 (part-time school) | 2A–2B (light–moderate aerobic) | Common clinic zone—sport may be “allowed” while school still formalized |
| 4 (full-time school) | 3 (individual sport-specific, no head impact) | Aerobic prescription often active; contact still off |
| 4 (full-time, no accommodations) | 4–6 (team drills → contact → play) | Amsterdam: high-risk sport after full RTL + exertional symptom clearance |
Document both coordinates. “Cleared to exercise” without an RTL label is an incomplete state vector.
Three operational disagreements (expanded)
Disagreement 1 — Sequence: Consensus text emphasizes school success before unrestricted sport PMID: 28446457 PMID: 37316210. DeMatteo’s cohort shows simultaneous early-stage progression is common and can be safe for non-contact phases PMID: 31396150. Chart data suggest RTP structured before RTL in many offices PMID: 35292472. What is actually contested is not “school first vs parallel ever” but where the hard gate sits (contact sport vs any activity) and who documents the school leg.
Disagreement 2 — Clocks: Meta means (~8 d RTL, ~20 d RTS) describe aggregated study endpoints in athletes PMID: 37316183. Youth medians (~35 / ~38 d) describe full protocol completion in one prospective sample PMID: 31396150. Quoting the fast number to reassure families while the school still runs a six-week accommodation plan misaligns expectations.
Disagreement 3 — Prescription attachment: Sub-symptom %HRmax (or RPE / symptom-cap) and minutes × days / weekly volume (~100 min/wk prescribed vs ≥160 min/wk observational bands PMID: 33856860) attach naturally to RTP step 2. Screen limits, exam deferrals, and partial days attach to RTL. If only the sport prescription is updated at follow-up, the family may stack cognitive and aerobic load on the same afternoon—symptoms spike, and both tracks blame the wrong lever.
Pragmatic trials comparing coordinated dual-track documentation with single-track RTP-focused follow-up—same-day symptom and adherence reporting on both legs, not only sport clearance—would test the first disagreement.
Cohort studies would help the second if they reported RTL step 1–4 and RTP step 1–6 dates in the same row, with symptom scores after combined daily load rather than separate sport-only exertion tests.
4. School, clinic, and home coordination
Intensity without BCTT and weekly-minute logging both leave open what happens when the school checklist and sport checklist are updated by different adults on different days.
Setting matrix (dual-track)
Setting A
School athletic trainer + classroom
- AT runs RTP steps; counselor/nurse holds RTL accommodations
- Clearance notes often sport-weighted
- School may not see HR band or walk prescription
Risk: RTP step 2 logged; RTL step 3 invisible on same plan
Setting B
Sports medicine clinic
- Visit note documents RTP; school forms lag
- May prescribe aerobic dose without calling school
- REAP / Living Guideline tools exist but are separate PDFs PMID: 26589561 PMID: 34777657
Default: export both step labels to school and coach same visit
Setting C
Primary care + parent supervision
- Parent hears “walk 20 minutes” from clinic
- School emails accommodation list separately
- No shared staging document
Default: one home log with RTL + RTP columns
Vignette
A 15-year-old JV guard took an elbow to the head under the basket 18 days into the winter season—still in the window where most adolescents recover, but already juggling missed labs, a team conditioning expectation, and midterm prep. After urgent-care clearance, three documents diverged:
Sports medicine follow-up (week 2) — discharge sheet: symptom-limited walk 15–20 min, 5 days/week, stop if symptoms rise ≥2/10 from walk start (symptom-cap path; no BCTT). Parent interprets this as permission to “get back in shape.”
School accommodation letter (week 2) — counselor lists RTL step 3 items: full attendance with rest breaks, tests deferred one week, no loud assemblies, PE excused, preferential seating away from overhead lights. Not a half-day schedule—many districts keep students in building while limiting cognitive load.
Athletic trainer team form (week 3) — checkbox “RTP stage 2: light aerobic exercise.” Coach reads this as green light for tomorrow’s pre-practice jog with the team. The form has no RTL column and no line for same-day homework load.
Wednesday: She completes a solo 18-minute walk after school (symptoms 2/10 → 3/10, acceptable). That evening she makes up a biology lab write-up (~50 minutes, laptop, bright screen)—symptoms 3/10 → 6/10 until bedtime. Thursday AM fog is worse; she sits out conditioning. Coach says she “failed RTP”; teacher notes she “was fine in class until she overdid exercise.”
Siloed narratives caused this, not a stopwatch error. Amsterdam’s mild-exacerbation rule applies to each activity class—but families experience one cumulative day PMID: 37316210. DeMatteo’s cohort reported 64% with school problems during recovery and 31% with grade drops even as activity stages advanced PMID: 31396150—the vignette pattern is common, not exotic.
Work through the plan in order.
Write both coordinates on one line: RTL 3 (full day + accommodations) · RTP 2A (solo light aerobic, not team conditioning yet)—not “stage 2” in isolation.
Gate sport advance on combined load: If screen or homework provokes >2/10 for >1 hour, hold RTP advance even when the walk was tolerated. Weekly product still matters: log minutes × days, not a ritual stopwatch—Howell’s ~100 min/wk prescription band (20 min × 5 d/wk) and, in the same cohort’s volume analysis, ≥160 min/wk as the stronger observational discriminator at one month PMID: 33856860. An 18-minute tolerated walk does not by itself miss those weekly bands. Today’s ceiling may still be schoolwork, not weekly math.
Separate exercise from team reintegration: Team jogs and passing drills belong to later RTP steps. A walk prescription from clinic is not the same as return to practice environment.
One communication touchpoint: AT, counselor, and parent receive the same sentence (see §5 template)—not three incompatible summaries.
What to tell the family: “The walk after school was fine. The lab on the laptop was too much the same day. We are pausing both tracks, not failing sport, until a day tolerates walk + normal homework without a late spike. Team practice waits.”
Clinician note: Purcell et al. list symptom burden, rest, age/grade, and course load as core return-to-school factors PMID: 29500251. Halstead emphasizes school environmental adjustments, not only attendance status PMID: 24163302. Aerobic prescription without those variables is a single-track note.
5. SOP checklist — dual-track documentation
Synthesizes CISG coordination rules, DeMatteo staging, Carson implementation warnings, and intensity/volume rules for education only PMID: 37316210 PMID: 31396150 PMID: 35292472 PMID: 32079897 PMID: 33856860.
One-page SOP (community default)
| Role | Checklist |
|---|---|
| Clinician | □ Record RTL step (1–4) and RTP step (1–6) on every note—not “progressing well” |
| □ State which track is limiting today (school / sport / both) | |
| □ Pair RTP step 2 with an intensity path (% band, RPE, or symptom cap) | |
| □ Pair weekly minutes × days—~100 min/wk prescribed (20 × 5); ≥160 min/wk observational band PMID: 33856860—when prescribing aerobic volume | |
| □ Hold RTP 4–6 until full-time school without concussion accommodations (Amsterdam youth gate) | |
| □ Send one clearance paragraph to school + coach + family with both labels | |
| School / counselor | □ Accommodation list maps to RTL step, not generic “concussion protocol” |
| □ Ask for RTP step before allowing PE, club sport, or conditioning | |
| □ Flag if athlete is in RTL 1–3 while team resumes non-contact training | |
| Athletic trainer / coach | □ No contact drills until written RTP ≥4 and clinician documents RTL 4 (or explicit exception) |
| □ Log symptoms after session; ask about same-day school load before clearing next sport step | |
| Parent / athlete | □ Home log: columns for RTL activity, RTP activity, peak symptom, duration >1 h? |
| □ Stop same-day stacking if combined load triggers >2/10 for >1 h | |
| □ “Cleared to run” ≠ “cleared for games” ≠ “full school day without breaks” |
Example one-line status (copy to letter)
RTL 3 (full day + breaks, tests deferred, PE excused, reduced screens) · RTP 2A (solo walk 15–20 min, symptom cap +2/10) · No team conditioning / no contact · Re-check in 7 d or sooner if walk + homework same day worsens symptoms >2/10 for >1 h.
flowchart LR subgraph school [RTL track] R1[Step 1-2 home/homework] --> R3[Step 3 accommodations] R3 --> R4[Step 4 full day no accommodations] end subgraph sport [RTP track] P1[Step 1-2 light aerobic] --> P3[Step 3 individual drills] P3 --> P4[Steps 4-6 team/contact/play] end R4 --> P4 P1 -.->|overlap allowed early| R3
Diagram: Early overlap (dotted) is permitted; high-risk sport (steps 4–6) waits on full RTL (step 4) per Amsterdam youth guidance PMID: 37316210.
Optional intensity helper: the standalone HR calculator encodes % bands—use as a ceiling within RTP step 2, not as permission to ignore RTL limits.
Important
Educational use only. Staging labels summarize published consensus and chart-review literature—they do not replace local return-to-play law, school board policy, or individual medical judgment.
6. Limitations
Step text paraphrased from CISG appendices; local policies and tools (REAP, SCHOOLFirst, Living Guideline) add detail not fully tabulated here PMID: 34777657 PMID: 35292473 PMID: 26589561.
North American chart-review dominance; “premature” RTL/RTP definitions vary by chart auditor and era PMID: 24925965 PMID: 35292472.
Marginal proportions: Carson relapse figures are not, in published form, a full set of conditional probabilities for individual counseling.
Abbreviation collision: DeMatteo RTS = school vs CISG RTS = sport persists in the literature—readers must translate, not merge PMID: 31396150 PMID: 37316210.
No adolescent PPCS RCT randomizing dual-track coordination vs sport-track-only follow-up with preregistered combined-load outcomes.
Aerobic PPCS evidence still sport-track weighted: Leddy-style subsymptom trials enroll exercise arms without parallel school-load manipulation PMID: 30715132—aerobic intensity/volume prescriptions may outpace RTL documentation.
Scope: Staging synthesis for documentation—not a substitute for school board policy or medical clearance.
What these limitations mean in practice
The most actionable gap is a missing shared row in the chart, not a missing seventh RTP stage. Until trials report both tracks with combined daily symptoms, clinics should treat dual-track staging as a documentation and communication problem first, and a prescription problem second. That is where %HR / RPE / symptom-cap bands and weekly minutes actually attach: inside labeled RTP steps, gated by RTL tolerance—not floating alone on a discharge sheet.
Berlin paired four RTL steps with six RTP steps in one consensus document PMID: 28446457. Amsterdam refined the symptom rules and made the parallel-track logic explicit PMID: 37316210. Canadian charts still show both tracks released too early, with RTL improvements lagging RTP PMID: 35292472. The literature does address coordination; the trouble is how easy it is to read one column and call it recovery.
Series: Foundation Stack · methods · RTL/RTP dual-track staging