Twenty Minutes From Where? Why Session Duration Is the Wrong Unit for Adolescent PPCS Prescription
Twenty minutes appears on every adolescent PPCS handout—but the number circulates by citation, not experiment. This methods piece maps that history, then where observational weekly-volume work comes closest to an answer.
Caution
Not medical advice. Educational use only. Data from published literature.
Every adolescent PPCS protocol I opened agreed on one surface detail: aerobic exercise should happen in bounded sessions—often around twenty minutes, often most days of the week. None of the papers I traced could answer the question a parent actually asks: Why twenty? Why not fifteen? Why not thirty?
That parent question is where the handout starts to look arbitrary.
Published protocols already fragment on testing and intensity anchors—treadmill thresholds, age-predicted %HR bands, RPE, symptom caps. Even after intensity is chosen, the prescription sheet still usually says something like “20 minutes, 5 days per week”—as if that pair were evidence-derived rather than inherited.
The “20 minutes” line on most handouts is thinner evidence than it looks. This piece traces how that number circulated, then follows observational work on weekly aerobic volume (minutes × frequency)—still imperfect, but closer to what the literature actually measures. Clinicians who need a schedule today should start with Section 4 and the SOP.
The useful question is not “What is the magic number?” but “What variable does the literature actually measure when it tries to relate exercise to symptoms?” Section 1 covers session duration; Section 2 covers weekly volume.
1. How “20 minutes, most days” became literature wallpaper
Buffalo-style subsymptom-threshold prescription pairs an individualized heart-rate target with a duration target—commonly about twenty minutes per day at sub-threshold intensity PMID: 31105634. Leddy et al.’s adolescent trials specify at least 20 minutes daily of subsymptom-threshold aerobic exercise for up to four weeks after injury PMID: 30715132 PMID: 34600629. Howell et al.’s YMCA branching-bike work instructs 5 days per week at prescribed intensity PMID: 35489100.
Those numbers look precise. They are also rarely experimentally compared against alternative session lengths in adolescent PPCS. No trial in the literature reviewed here randomizes 15 versus 20 versus 30 minutes while holding weekly volume constant. Duration is assumed, not tested.
Montreal active-rehabilitation protocols cap supervised aerobic work at 15 minutes per session in the 50–60% target zone PMID: 29058559 PMID: 25735821. Kurowski’s Pittsburgh SE trial individualized duration as 80% of the time that provoked symptoms during testing, up to 30 minutes, on five to six days per week PMID: 27120294. Micay’s fixed-bike protocol began at 10 minutes and progressed toward 20 minutes over the first week, on a two-days-on, one-day-off schedule PMID: 30305924. Chrisman et al.’s MSTEP protocol starts youth at 10 minutes per day and advances toward 60 minutes per day of moderate-to-vigorous activity to meet U.S. federal MVPA recommendations PMID: 35473570.
Authors disagree widely on session length, but they rarely argue for their choice with experiment—what repeats is citation, not derivation.
Chrisman et al. justify advancing toward 60 minutes per day by citing U.S. MVPA guidelines PMID: 35473570—a different justification chain entirely (population health recommendations grafted onto PPCS telehealth). Kurowski justify four-week benefit assessment within a six-week program because benefits appeared largest around four weeks PMID: 27120294. Those are program-architecture choices, not session-length experiments—but they shape what clinicians copy onto prescription pads.
Howell et al. (2021) make the circularity visible in a single sentence when explaining their 100 min/week grouping:
“This classification was done based on our prescription to the intervention group to exercise 20 min/d for 5 d/wk, consistent with previous studies.” PMID: 33856860
They immediately add that while prior work suggests 100 minutes per week may suffice for adolescents who already have persistent symptoms, the dose necessary for beneficial effects in acute and subacute phases remains unknown—the same paper that later reports ≥160 min/week as a stronger discriminatory threshold for symptom resolution at one month.
This reflects less on Buffalo or Howell specifically than on how a field bootstraps operational parameters before dose-response trials exist. Clinicians inherit the result as “20 minutes” on a handout. The handout rarely says the number is conventional, not validated.
Reading the spread: session length is not one number
Tracing the citation chain reveals a collective convention: authors justify session length by pointing to prior studies that justified session length by pointing to earlier studies. The table below is the deconstruction endpoint—evidence of chaos, not a new prescription. When you multiply stated duration by stated frequency, “20 minutes” protocols do not even agree on weekly product.
Table note: “Weekly volume” multiplies stated session duration by stated frequency when both are fixed in the source. “Duration varied in trial?” asks whether session length was a manipulated experimental factor—not whether duration changes within a prescribed progression.
| Source / protocol line | Session duration | Frequency | Implied weekly volume | Duration varied in trial? | PMID |
|---|---|---|---|---|---|
| Buffalo BCTT prescription | ~20 min at target HR | Daily | ~140 min/wk | No | PMID: 31105634 |
| Leddy adolescent RCTs | ≥20 min subsymptom | Daily | ≥140 min/wk | No | PMID: 30715132 PMID: 34600629 |
| Howell YMCA bike (prescription) | 20 min at target HR | 5 d/wk | 100 min/wk | No | PMID: 35489100 |
| Montreal active rehab (Dobney) | ≤15 min | Daily | ≤105 min/wk | No | PMID: 29058559 |
| Kurowski Pittsburgh SE | Up to 30 min (80% symptom time) | 5–6 d/wk | Variable | Individualized, not compared | PMID: 27120294 |
| Micay fixed bike | 10 min → 20 min (wk 1) | 2 on / 1 off | ~47–93 min/wk (est.) | Fixed schedule | PMID: 30305924 |
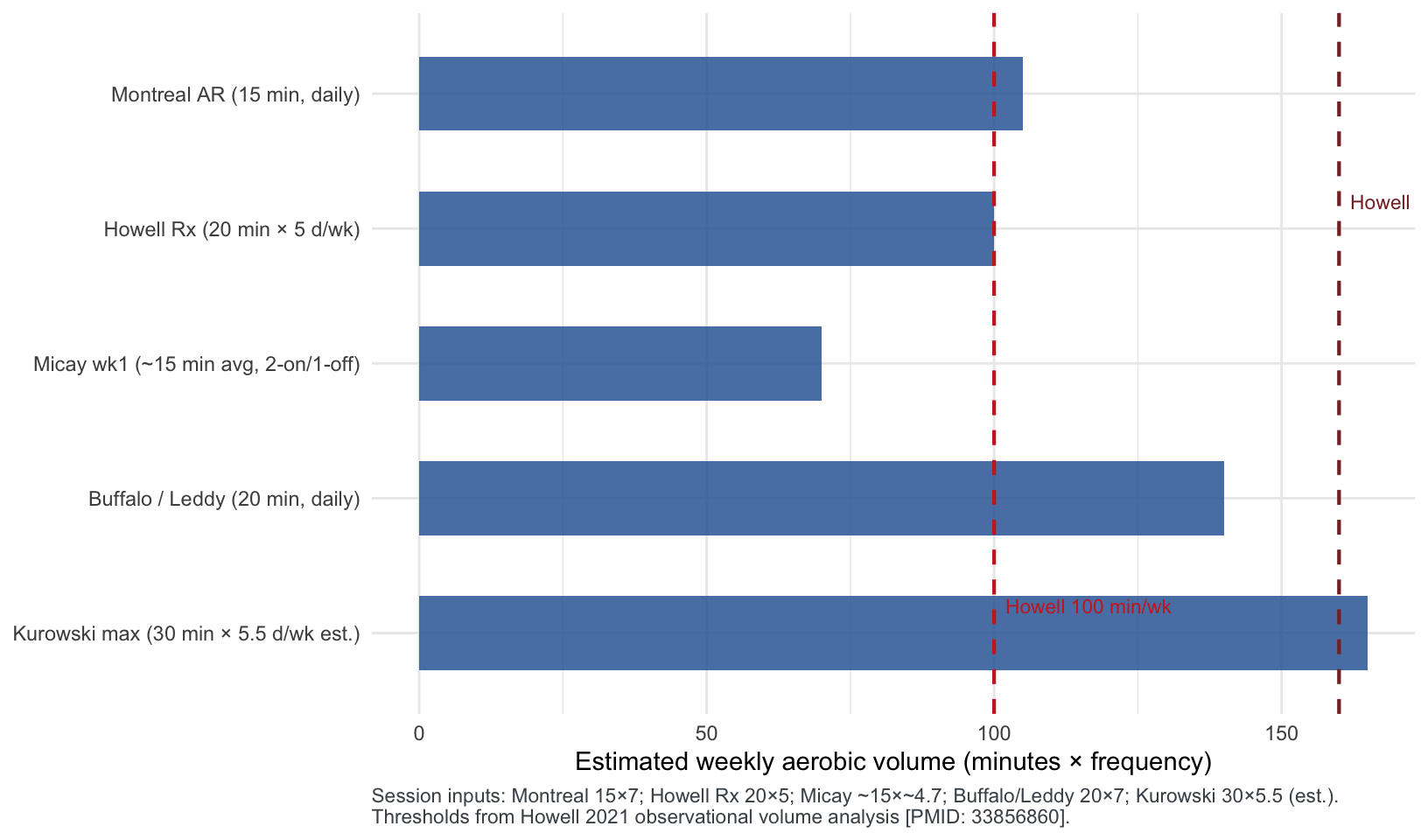
Figure 1 — Session length vs weekly volume
Figure 1. Bars show estimated weekly volume (minutes × frequency), not single-session duration. Dashed lines preview Howell 2021 volume bands discussed in Section 2.
Pattern A — Different sessions, similar weeks. Fifteen minutes daily (~105 min/week) and twenty minutes five days per week (100 min/week) land in the same neighborhood. A parent told they “failed” because a walk lasted eighteen minutes instead of twenty may be enforcing ritual precision the literature never validated.
Pattern B — Progressive duration ≠ dose experiment. MSTEP’s march toward 60 minutes per day PMID: 35473570 and Micay’s session-length ramp PMID: 30305924 change duration over time within a protocol. That is titration logic, not proof that 20 minutes is the uniquely correct session length at every week.
2. What the literature measures instead: weekly volume
If session duration were the causal lever, trials would manipulate minutes per session. What the library contains instead is volume observational work: researchers measure how much aerobic activity accumulated—often by self-report or actigraphy—and relate totals to symptoms.
Howell et al., 2021 (American Journal of Sports Medicine). In adolescents tested within two weeks of injury, randomization to a structured prescription did not cleanly separate exercise volume from standard care—many control participants also exceeded 100 min/week once active rehabilitation became usual practice PMID: 33856860. Collapsing groups by reported volume, those exercising <100 min/week during the first study month reported higher symptom severity at one month than those at ≥100 min/week. A receiver-operating-characteristic analysis identified ≥160 min/week as a cutoff that discriminated symptom-free versus symptomatic participants at one month with 81% classification accuracy (90% sensitivity, 78% specificity)—better than the 100 min/week prescription line alone.
The authors caution this is a secondary, retrospective analysis: adolescents who felt better may have exercised more, not only the reverse. Still, the paper’s central operational insight stands: weekly volume tracked outcome variation more convincingly than assignment to a 20-minute prescription label.
Wingerson et al., 2024 (Medicine & Science in Sports & Exercise). Among adolescents and young adults in an aerobic exercise intervention, those whose symptoms resolved within 28 days showed longer average session duration and greater adherence than non-resolvers PMID: 38109187. Session frequency alone did not separate groups—suggesting that how much total work gets done, and whether prescribed sessions actually happen, may dominate a rigid “5 days per week” checkbox.
The same reverse-causality caveat as Howell 2021 applies: adolescents who were already easing may have tolerated longer sessions because symptoms were improving—not only the reverse. Adherence still matters operationally—families who cannot complete prescribed sessions never test any volume hypothesis—but longer sessions are not proof of causation.
Neely et al., 2023 (PM&R). In a prospective observational cohort tracked with actigraphy in the weeks after injury, fewer exercise sessions per week increased odds of persistent symptoms beyond 28 days. Completing more sessions lasting >15 minutes was associated with reduced PPCS risk PMID: 36580488. Frequency and session-length thresholds interact: a week of three long walks and a week of five short walks are not interchangeable even if a naive minute product looks similar.
Actigraphy reduces recall bias relative to self-report, but directionality remains ambiguous: persistent symptoms may suppress session completion rather than the reverse. Neely’s >15 minute threshold is still worth documenting—it separates a deliberate aerobic block from incidental movement—even before causation is settled.
Howell & Wingerson, 2024 (Journal of Head Trauma Rehabilitation) — sleep outcome, not symptom dose. Adolescents who accumulated >150 min/week of actigraphy-recorded aerobic exercise showed greater Pittsburgh Sleep Quality Index improvement than those at ≤150 min/week PMID: 38032838. Treat this as related but distinct: sleep quality matters in PPCS, but the 150-minute band is not interchangeable with Howell 2021’s 160-minute symptom ROC without over-reading observational cutoffs.
Three operational disagreements
Disagreement 1: Session length vs weekly product
Protocols anchor clinician attention on per-session minutes because sessions are easy to script. Volume studies suggest minutes × frequency is the construct associated with outcomes. No head-to-head trial holds weekly volume constant while varying only session length in adolescent PPCS.
Disagreement 2: Prescription threshold vs discriminatory threshold
Howell’s 100 min/week reflects what the trial prescribed (20 × 5). The 160 min/week line reflects what actually separated symptom-free adolescents in post hoc analysis. Clinicians who treat 100 as ceiling and 160 as aspirational—or who conflate the two—risk mis-calibrating family expectations.
Disagreement 3: Supervised trial volume vs home execution
Kurowski’s Pittsburgh SE trial reported lower adherence in the aerobic arm than stretching yet faster symptom improvement—reminding readers that logged volume in trials still exceeds most home programs PMID: 27120294. A weekly-dose framework helps only if someone measures volume honestly (diary, actigraphy, or structured school sessions)—not if “20 minutes” lives only on a discharge sheet.
Until a factorial trial holds weekly volume constant while varying session shape, I would still prescribe in weekly-minute bands—Howell’s 100 min/week as the documented prescription line, 160 min/week as an aspirational observational band, not a second prescription—and flex session length to the school week. Wednesday at thirty minutes plus two shorter walks beats stopwatch guilt over “not twenty.”
Reporting standards that require both prescribed and achieved weekly minutes in PPCS trials—including control arms receiving “standard care” active rehabilitation—would sharpen the second disagreement over time; they do not change what to measure this month.
3. From single session to weekly total: what the reframe changes
Section 1 showed that “twenty minutes” is conventional, not experimentally chosen. Section 2 showed that when outcomes are stratified at all, they stratify on weekly aerobic volume—imperfectly and associatively, but consistently enough to matter clinically.
The single most useful takeaway for prescribers is Disagreement 2 from Section 2: 100 min/week is what Howell prescribed (20 × 5, “consistent with previous studies” PMID: 33856860); 160 min/week is what separated symptom-free adolescents in the same paper’s post hoc analysis. Those are not interchangeable targets—and collapsing them is how families inherit stopwatch guilt over a digit the literature never validated session-by-session.
That distinction does not replace intensity rules—age-predicted %HR, RPE, or a ≥2/10 symptom rise stop. It does mean the negotiable unit becomes minutes × days per week, logged honestly, with symptom caps intact. Section 4 walks through what that looks like when a parent texts ”We failed the protocol.”
4. Applying the volume reframe at home
Intensity without BCTT is one problem; volume without worshipping a single session template is another—especially when school athletic trainers and home / primary-care supervision face different scheduling realities.
Vignette
A 14-year-old ninth grader has headache and fatigue six weeks after a header in practice. Both parents work until 6 p.m. No treadmill at school; the athlete walks the family dog alone after school—about twenty minutes on most weekdays, unsupervised. The discharge sheet says “20 minutes aerobic exercise, 5 days per week.” Last Tuesday the walk was eighteen minutes because the dog stopped early; the mother texted the school nurse: “We failed the protocol.”
This is a home / primary-care supervision setting. Intensity was never BCTT-anchored; the family uses a symptom cap (stop if headache or fog rises ≥2/10 from walk start) and brisk walking pace—full sentences, no breathlessness.
Volume reframe applied:
Eighteen minutes is not a protocol failure. At ~20 min × 5 d/wk, the weekly product is ~100 min/week—the same neighborhood as 15 min × 7 d/wk. The literature never validated the stopwatch digit; it validated (loosely) weekly accumulation PMID: 33856860.
Unsupervised execution is the real constraint. Wingerson 2024 links adherence and session length to resolution PMID: 38109187. A plan the teen can repeat without a parent clocking every minute beats a perfect Buffalo handout no one completes.
Schedule negotiation. If soccer practice consumes two weekdays, three longer weekend walks (25–30 min, sub-symptom) may approach the same weekly band as five school-day dog walks—use the weekly dose helper to compare products before changing intensity.
What to tell the family: “We care about roughly a hundred minutes this week, walking fast enough to talk in sentences but not gasping. If Tuesday is eighteen minutes, that is fine. If symptoms jump more than two points, stop—do not add minutes to ‘make twenty.’ Missing Friday does not mean doubling Saturday.”
Clinician note: Revisit if <100 min/week persists two weeks with stalled symptoms, or if walks are symptom-limited because intensity (pace, hills) is too high—not because the timer is wrong.
Schedule arithmetic (educational)
| Schedule | Minutes × frequency | Weekly volume | Howell 100 | Howell 160 (ROC) |
|---|---|---|---|---|
| Short daily walks | 15 min × 7 d/wk | 105 min/wk | Met | Below |
| Buffalo-style handout | 20 min × 7 d/wk | 140 min/wk | Met | Below |
| Classic trial prescription | 20 min × 5 d/wk | 100 min/wk | Met (exact) | Below |
| Alternate school week | 30 min × 3 d/wk | 90 min/wk | Below | Below |
| Longer weekend sessions | 25 min × 6 d/wk | 150 min/wk | Met | Below |
The table is arithmetical, not outcome-proven. It shows why a family that can only supervise three after-school walks might need longer sessions to approach observational bands—not because thirty minutes is magic, but because 100–160 min/week is a product.
For parents, the translation shifts from “Was it exactly twenty minutes?” to “Did we accumulate roughly a hundred minutes this week without symptom spikes—and did every session stay sub-symptom?” That pairs naturally with a ≤2/10 stop rule and 24-hour advancement logic.
5. SOP checklist and weekly-dose tool
One-page SOP (volume-aware community default)
Synthesizes Howell 2021 volume findings, Neely 2023 session-frequency data, and symptom-cap stop rules for education only PMID: 33856860 PMID: 36580488 PMID: 30742254.
| Clinician | Parent | Adolescent |
|---|---|---|
| □ Document minutes × days/week achieved, not only “compliant yes/no” | □ Log each session’s duration and peak symptoms | □ Rate symptoms 0–10 before and after every walk or bike session |
| □ Pair volume with an intensity path (%, RPE, or symptom cap) | □ Weekly total matters more than one “failed” short session | □ Stop if symptoms +2/10 from session start—do not extend minutes to “hit twenty” |
| □ Discuss 100 vs 160 min/wk as observational bands, not guarantees | □ Shorter daily walks can equal one long Buffalo-style session across the week | □ Missing a day → recover schedule without doubling duration same day |
| □ Use diary or wearable if available; actigraphy studies used objective totals PMID: 36580488 | □ Report sessions >15 min when updating clinician (Neely threshold) | □ School days count—commute walks can add volume if sub-symptom |
| □ Revisit prescription if <100 min/wk persists two weeks with stalled symptoms | □ Ask whether fatigue is from under-dosing or over-intensity, not wrong clock time | □ No contact sport without written clearance |
Weekly-dose helper (educational tool)
Published %HRmax fallback bands do not converge on one intensity number. This piece’s claim is different—weekly totals may have observational thresholds even when session length does not. The standalone weekly dose helper multiplies minutes per session by sessions per week and maps the product to published bands (Howell 100 and 160 min/week; sleep-related 150 min/week flagged separately).
Use it to compare schedules—for example, whether 15 minutes × 7 days and 20 minutes × 5 days land in the same weekly band—not to override symptom caps or intensity rules.
Important
Educational use only. Thresholds come from observational secondary analyses and actigraphy cohorts—not from a preregistered dose-finding RCT in adolescent PPCS.
6. Limitations
No session-length RCT: The library lacks a trial that manipulates only per-session duration while holding weekly volume constant in adolescent PPCS.
Circular prescription history: The 20-minute convention propagates by citation PMID: 33856860; no derivation exists in the literature to invent.
Retrospective volume analyses: Howell 2021’s 160 min/week ROC and Neely 2023’s session counts are associative; directionality (exercise → symptoms vs symptoms → exercise) remains ambiguous.
Acute vs persistent populations: Howell 2021 enrolled within 14 days of injury; extrapolation to slow PPCS at six weeks requires caution—overlapping clinical audience, not identical evidence.
Intensity unmeasured in volume bands: Weekly minutes without sub-symptom intensity context can over-dose if walks are too fast or under-dose if sessions are symptom-limited but brief.
Adherence: Wingerson 2024 links adherence and session duration to outcomes PMID: 38109187; a weekly-minute framework does not solve unsupervised execution—trial adherence often exceeds what home programs achieve PMID: 27120294.
Scope: Weekly-volume synthesis for education—not a substitute for individualized medical assessment or preregistered dose-manipulation trials.
What these limitations mean in practice
Treating 20 minutes as folklore rather than physics does not mean volume is destiny. It means clinicians can negotiate schedules with families—shorter daily sessions, fewer longer sessions—while tracking weekly sub-symptom aerobic exposure honestly. Until dose-manipulation trials exist, transparency about which band you are targeting (prescription 100, discriminatory 160, or neither) is part of good clinical communication—not optional fine print.
Session duration is the most copied number in adolescent PPCS aerobic prescription—and the least defended. Montreal caps at fifteen minutes; Buffalo and Leddy ask for twenty; Kurowski permits up to thirty; MSTEP aims for sixty on a public-health timeline PMID: 29058559 PMID: 31105634 PMID: 27120294 PMID: 35473570. Observational dose work suggests the weekly integral may matter as much as any single session’s stopwatch reading PMID: 33856860 PMID: 36580488.
The field inherited both numbers the same way Howell admitted grouping them: “20 min/d for 5 d/wk, consistent with previous studies.” PMID: 33856860 Session length circulated by citation; the weekly product followed. Volume observational work does not close that ring—it names what to measure until dose-manipulation trials exist.
Series: Foundation Stack · methods · exercise dose / weekly volume