No Treadmill in the Room: Prescribing Sub-Symptom Aerobic Exercise Without BCTT
foundation-stack
PPCS
methods
aerobic-prescription
no-bctt
When symptom-threshold treadmill testing is unavailable, published protocols fall back to bike tests, field exertion, age-predicted heart-rate bands, and RPE anchors—but they do not agree. What follows compares those paths and shows how one educational tool encodes the fallback logic.
Caution
Not medical advice. Educational use only. Data from published literature.
Reviewing which heart-rate percentages clinicians actually write when a treadmill is unavailable, I kept finding the same thing: not a number, but a range—and the ranges overlapped without converging. 50–60% in one review. 60–75% in a structured trial. Borg 11 on a bike in another. All cited as fallback. None citing each other.
Six major adolescent PPCS protocols already disagree on testing. Buffalo wants a treadmill. Toronto wants qualitative pacing. NICE wants symptom caps in primary care. Pittsburgh SE wants supervised graded work in hospital PT. Berlin wants six stages and a 24-hour rule. Symptom-limited approaches want observation, not equipment.
The question that actually arrives in clinic is narrower: what do you do when there is no treadmill in the room?
Not hypothetically. A school athletic trainer three weeks post-injury. A community pediatrician whose referral queue to sports medicine is measured in weeks. A rural PT with a bike ergometer but no Buffalo protocol training. A parent at home with a wrist-worn heart-rate monitor and a teenager who still has headache at the end of the school day.
The literature does not answer with silence. It answers with a patchwork—bike protocols, field shuttle runs, YMCA branching tests, age-predicted heart-rate bands, Borg scales, and symptom caps that never required a device in the first place. Each path trades precision for deployability in a different way.
What follows compares those compromises: what each path assumes, where the bands overlap, where they contradict each other, and how three common settings should choose among them. A short educational tool section shows how one published R package encodes the age-predicted fallback when HRt is unknown—illustration only, with GRADE LOW certainty on the underlying evidence.
1. Why “no BCTT” is a distinct problem, not a minor inconvenience
Buffalo-style prescription assumes you can measure a symptom threshold heart rate (HRt) on a treadmill and prescribe at roughly 80% of that number PMID: 31105634. That assumption holds in university sports medicine clinics with trained staff, weekly follow-up, and a culture built around graded exertion testing. It often fails everywhere else.
School athletic trainers, community pediatricians, and rural physical therapists frequently face the same patient profile: an adolescent with lingering post-concussive symptoms, parents asking when exercise can resume, and no treadmill in the building. Referral to a BCTT-capable center may mean weeks of delay. Meanwhile, published guidance still recommends sub-symptom-threshold aerobic exercise—not strict rest PMID: 33147117.
On whether exercise helps, the adolescent PPCS literature has grown substantially more consistent over the past decade. The real gap is how to set the first target when you cannot run the test that Buffalo, Pittsburgh SE, and much of the RCT literature were built around.
Reviews acknowledge the problem directly. McIntyre et al. note that when graded exercise equipment is unavailable, targeting 50–60% of age-predicted maximum heart rate appears safe and practical PMID: 32079897. That is useful—but it is not a unified standard. Hutchison’s structured aerobic exercise protocol (SAEP) progressed from 60% toward 75% age-predicted maximum over eight sessions in the first week post-injury PMID: 36256698. Kurowski’s Pittsburgh SE work anchored prescription to Borg RPE ≈11 on a bike rather than a measured HRt PMID: 27120294. Micay began fixed bike work at 50% and added 5% per session PMID: 30305924.
For the slow-to-recover adolescent in a resource-limited setting, the cost of this ambiguity is practical. The adults in the room must pick a path without a shared decision framework—the same protocol-level fragmentation, now compressed into a single visit.
There is a second layer: access inequality disguised as protocol choice. When the “correct” protocol requires equipment and expertise that most adolescents cannot reach within two weeks of the decision point, the literature’s gold-standard path becomes a deferral strategy. The patient exercises under no protocol, or under whatever fragment a parent found online, while waiting for the appointment that may never be convenient. Mapping no-BCTT paths is the operational reality for a large fraction of real-world care, not an academic exercise in secondary options.
A third layer is timing. Chizuk et al. published a standardized aerobic program explicitly for adolescents in the absence of graded exercise testing PMID: 36728783—acknowledging that many outpatient clinicians will never have a treadmill in the room but still need a defensible prescription on visit one. Teel et al.’s MOVE protocol pushes exertion grading into remote, bodyweight-based levels for settings where even bike ergometry is scarce PMID: 36580652. Rather than waiting for universal BCTT access, the literature offers parallel rails, each with different evidence weight and different supervision demands.
Finally, there is a communication problem inside the no-BCTT cluster itself. Two clinicians can both reject Buffalo’s treadmill requirement and still disagree: one prescribes 55% age-predicted maximum with a chest strap; another prescribes Borg 11 on a bike; a third tells the family to walk until symptoms stay under a 2-point cap. All three can cite papers. None is necessarily wrong. The adolescent experiences that as whiplash—the same failure mode across six major protocols, now reproduced inside the fallback literature.
2. Fallback paths compared
Table note: Paths below are substitute or fallback routes when BCTT is unavailable or inappropriate—not a ranking. “Typical anchor” summarizes what each source actually prescribes; bands often overlap without agreeing on a single percentage.
| Path | Test required | Typical intensity anchor | Progression | Typical setting | Source |
|---|---|---|---|---|---|
| BCTT (reference) | Treadmill, graded | 80% HRt, ~20 min/day | Weekly retest; advance when HRt rises | Sports medicine clinic | 31105634 |
| BCBT | Stationary bike, graded | HRt from bike test → ~80–90% prescription | Same logic as BCTT; head/neck more stable | Clinic; vestibular-sensitive patients | 31488375 |
| YMCA branching bike | Bike, submax protocol | Branching watts by % age-predicted HR | Fitness-adjusted stages | Cerebrovascular / research lab | 35489100 |
| mSRT (field) | Modified shuttle run | Exertion level vs prior BCTT validation | Field administration | School gym, large groups | 35894897 |
| Age-%HRmax band | None (formula) | 50–60% to 60–75% age-predicted max (studies disagree) | Fixed steps or time-based | Home, school, community | 32079897 36256698 29058559 |
| RPE-anchored | Often bike; no HRt required | Borg ~11 (Kurowski); complement HR in reviews | PT-supervised titration | Hospital / outpatient PT | 27120294 36940683 |
| Symptom cap only | None | ≤2/10 symptom increase vs baseline | ≥24 h without escalation | Any setting with observation | 30742254 |
| MOVE / remote grading | Bodyweight levels | Graded exertion vs BCTT equivalence | Remote follow-up | Telehealth / home | 36580652 |
Reading the table: three clusters
Cluster A — Measured threshold, different equipment. BCBT, YMCA branching bike, and mSRT still produce a physiological anchor. They change the equipment and environment, not the logic of threshold-based prescription. Haider et al. demonstrated that HR at symptom exacerbation on the BCBT is equivalent to the BCTT in acutely concussed adolescents—a clinically important finding for sites with bikes but no treadmills PMID: 31488375. Howell et al. explicitly chose stationary cycling because treadmill movement artifact and vestibular provocation can distort assessment in acute concussion PMID: 35489100. Miutz et al. position the modified shuttle run as a field alternative when lab BCTT is impractical at scale PMID: 35894897.
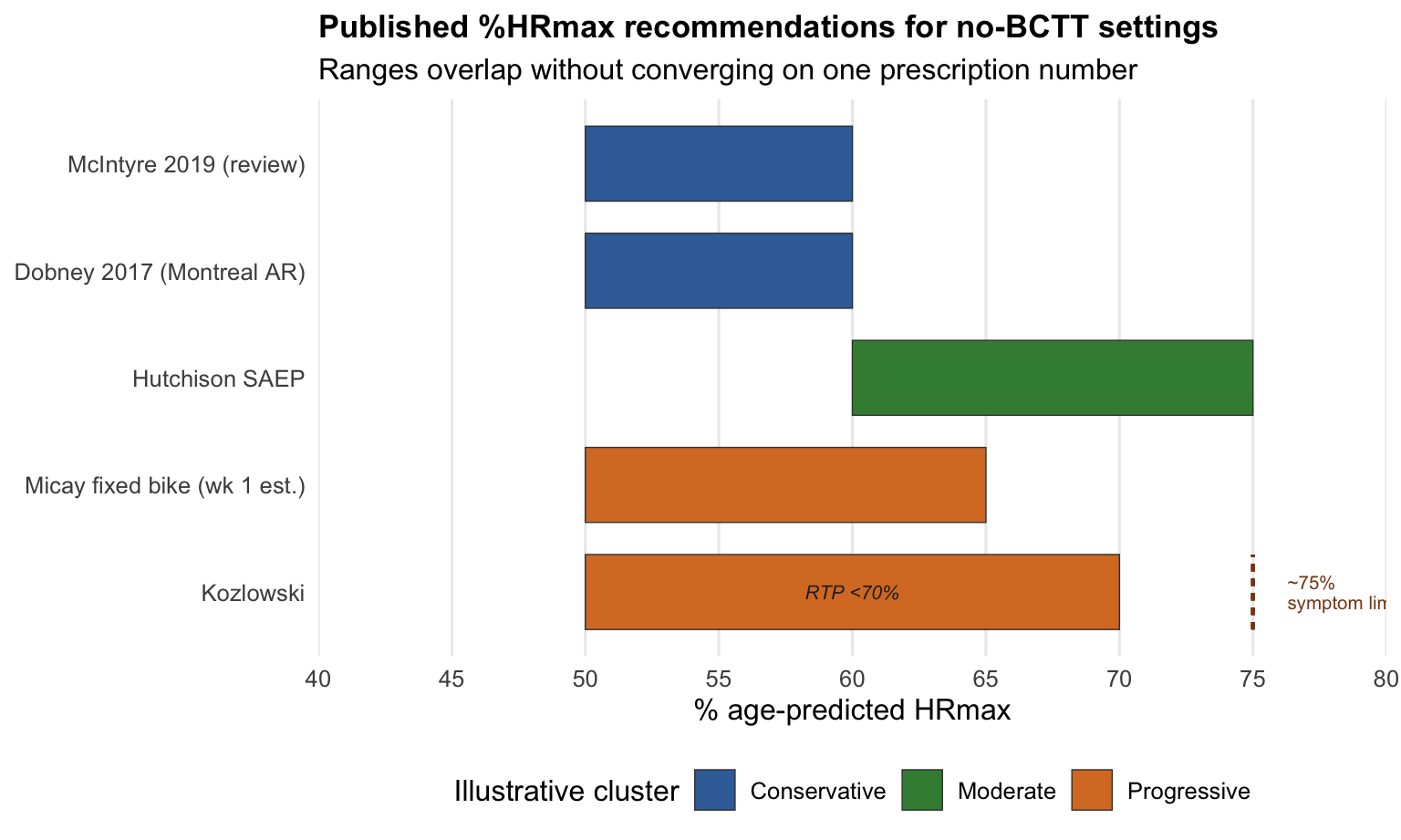
Cluster B — Formula fallback. When no graded test is available, authors default to age-predicted percentages. The bands overlap (roughly 50–70%) but do not converge on one number. McIntyre: 50–60% PMID: 32079897. Montreal active rehabilitation (Dobney et al.): 50–60% target zone for 15 minutes on bike or treadmill PMID: 29058559 (figure cited from full text; intensity data not in abstract). Hutchison SAEP: structured progression from 60% upward PMID: 36256698. Kozlowski: persistent PCS patients reached ~75% age-predicted maximum at symptom limit—supporting RTP guidance to stay below 70% when threshold is unknown PMID: 23952041.
Figure 2 — Overlapping %HRmax bands (Cluster B)
Figure 2. Bars show published targets or progression bands (not equivalent constructs). Micay: initial 50% with +5% per session (bar = first-week span to ~65%). Kozlowski: orange bar = RTP guidance to stay below 70% when HRt is unknown; dashed line = ~75% age-predicted maximum at symptom limit in persistent PCS PMID: 23952041. Colors = illustrative clusters (conservative / moderate / progressive), not author-defined tiers.
Cluster C — Symptom-only. Symptom-limited walking or cycling—stop when symptoms rise about ≥2/10 from session start—remains the most deployable path when neither equipment nor reliable heart-rate monitoring exists PMID: 30742254. It trades precision for accessibility.
Castellana et al. offer a bridge between Buffalo and formula worlds: in adolescents, prescriptions at 80% vs 90% HRt both mapped to “light effort” (about 50–63% age-appropriate max HR) for 15-year-olds—suggesting measured and age-band approaches may land in a similar perceptual zone even when numerically different PMID: 38980666. That observation does not resolve the disagreement; it explains why clinicians sometimes report that formula-based home programs “feel about right” compared to clinic-derived Buffalo prescriptions.
One row deserves explicit caution: 6MWT and distance walk tests. A structured search of the adolescent PPCS aerobic literature found no six-minute walk test validation in concussion prescription. Clinicians sometimes reach for field walks because they are familiar from cardiac rehab. That familiarity should not be mistaken for SRC-specific evidence. When a hallway is all you have, the honest mapping is to symptom-capped walking or structured remote grading (MOVE), not to an unvalidated distance target pulled from another discipline.
Figure 3 — Evidence matrix (what each path actually requires)
Legend: ● = directly supported in adolescent SRC/PPCS literature; ◐ = partial / proxy evidence; — = not required
| Requirement | BCTT | BCBT | YMCA bike | mSRT | Age-% | RPE | Symptom only | MOVE |
|---|---|---|---|---|---|---|---|---|
| Treadmill | ● | — | — | — | — | — | — | — |
| Stationary bike | — | ● | ● | — | ◐ | ◐ | — | — |
| Graded test staff | ● | ● | ● | ◐ | — | ◐ | — | ◐ |
| HR monitor | ● | ● | ◐ | ◐ | ◐ | ◐ | — | — |
| Age formula | ◐ | ◐ | ● | ◐ | ● | — | — | — |
| Symptom diary | ● | ● | ● | ● | ● | ● | ● | ● |
| Weekly clinic visit | ● | ● | ◐ | ◐ | — | ● | — | ◐ |
| Requirement | BCTT | BCBT | YMCA bike | mSRT | Age-% | RPE | Symptom | MOVE |
|---|---|---|---|---|---|---|---|---|
| Treadmill | Yes | — | — | — | — | — | — | — |
| Stationary bike | — | Yes | Yes | — | Opt | Opt | — | — |
| Trained tester | Yes | Yes | Yes | ◐ | — | ◐ | — | ◐ |
| HR monitor | Yes | Yes | ◐ | ◐ | ◐ | ◐ | — | — |
| Symptom diary | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Adolescent validation | Strong | Strong | ◐ | ◐ | ◐ | ◐ | ◐ | ◐ |
The matrix is a matching tool, not a quality score. A school with a bike and a trained AT using BCBT instead of BCTT is matching infrastructure to the patient, not failing. A home-only setting using symptom caps because monitoring is unreliable is acknowledging what can actually be observed.
3. Three operational disagreements
Disagreement 1: Which %HRmax band when HRt is unknown?
McIntyre’s review endorses 50–60% age-predicted maximum when BCTT equipment is unavailable PMID: 32079897. Montreal active-rehabilitation work used a 50–60% target zone on bike or treadmill for 15 minutes PMID: 29058559. Hutchison’s SAEP trial progressed from 60% toward 75% over eight sessions in the first week post-injury PMID: 36256698. Micay’s fixed bike protocol began at 50% and added 5% per session PMID: 30305924.
Nobody disagrees that sub-symptom aerobic exercise is reasonable. The disagreement is over which single number a clinician should write down when the evidence supports a range. No adolescent PPCS trial validates one universal percentage against a gold-standard HRt in community settings.
Clinically, this matters because parents ask for a number. “Walk until symptoms stay under control” is correct but vague. “Keep heart rate around 130” is actionable but evidence-ambiguous. The honest clinical communication is a band with a stop rule, not false precision: start conservative (often the lower half of the published overlap zone), monitor symptoms every session, and advance only when the 24-hour rule is satisfied.
Disagreement 2: Which test substitute—bike, field, or neither?
Bike proponents emphasize vestibular and movement-artifact advantages PMID: 35489100 PMID: 31488375. Field proponents emphasize throughput and access PMID: 35894897. Symptom-cap proponents emphasize that parents already detect symptom flare without any test PMID: 30742254.
Glendon et al.’s acute rugby cohort used BCBT or BCTT within a controlled early-exercise pathway PMID: 38910338. Early exercise intolerance in that study was associated with slower return to play and greater vestibular-ocular burden in the first days—supporting the value of some graded assessment, not necessarily the treadmill specifically.
The operational question for a school AT is concrete: Do I have a bike, a flat hallway, or only a symptom diary? mSRT is a validated field protocol in research contexts PMID: 35894897, but that validation doesn’t license sending a concussed adolescent on an unsupervised beep test in the gym. Unstructured home walking is symptom-limited exercise, a different thing from mSRT.
Disagreement 3: Which age formula—and does it matter clinically?
Most fallback paths implicitly use 220 − age as the denominator. The formula’s limitations for youth populations are discussed in the section below.
See: A note on the formula itself.
Jaganathan et al. add a parallel axis: when any HR anchor exists, Borg RPE should complement HR, not replace symptom monitoring PMID: 36940683. That is particularly relevant after concussion, when HR and perceived exertion can dissociate during recovery PMID: 27812398.
A note on the formula itself
Most fallback paths inherit 220 − age as the denominator. Pediatric exercise literature—including work on active rehabilitation intensity bands in adolescent concussion PMID: 29058559 and reviews noting that 208 − 0.7 × age fits youth better than 220 − age—suggests the classic formula can overestimate maximum heart rate in children and adolescents. At age 15, the difference is approximately 5–7 bpm: modest in absolute terms, but meaningful when the clinical goal is to prescribe a narrow band below symptom threshold.
Neither formula has been validated in adolescent PPCS specifically. The practical implication: any age-predicted band should be treated as an upper bound, not a precision target. When 220 − age is the denominator, 50–60% of an inflated HRmax may still fall within a safe zone—but the margin for error is smaller than the formula implies, and clinicians in settings with unreliable monitoring should weight symptom response more heavily than the calculated number.
For bpm conversion with published-band context, use the standalone HR prescription helper (ceiling not goal; does not resolve which % to choose).
Until a pragmatic trial compares BCTT-anchored 80% HRt, a fixed 55% age-predicted band, and symptom-cap-only progression—with adherence and symptom trajectory measured equally across arms—the defensible posture is transparency: state which anchor you used, note that the band is consensus-adjacent rather than individually measured, and document symptom response session by session.
Head-to-head equivalence trials of BCBT vs BCTT vs mSRT in the same acute and PPCS cohorts—with prespecified prescription rules, not only threshold detection—would sharpen the second disagreement. Haider’s equivalence work addresses threshold measurement PMID: 31488375; Miutz addresses field practicality PMID: 35894897. The prescription step after the test remains protocol-specific.
Better reporting would help the third: if trials published the HRmax formula, device type, and whether parents supervised sessions, clinicians could map evidence to setting with less guesswork. Today, many abstracts present clean percentages without the engineering underneath.
4. Three settings, three defaults
Foundation Stack value in this section: match path to infrastructure, not to whichever trial had the largest sample size.
Figure 4 — Three settings, three default paths
Setting A
School athletic training room
- No treadmill; referral wait 2–4 weeks
- Can supervise short sessions after school
- Often has bike or hallway access
Default path: Symptom cap + age-% band, or BCBT if bike/staff available
Setting B
Outpatient PT / community clinic
- Bike ergometer; periodic visits
- Can run submax or BCBT-style test
- May see PPCS at 4–16 weeks
Default path: BCBT or RPE-anchored bike (Kurowski-style)
Setting C
Home / primary care only
- No graded test; parent supervision
- Variable monitor quality
- Needs plain-language stop rules
Default path: Symptom cap ≤2/10; optional 50–60% if monitor reliable
The decision tree below maps the same logic before the vignette walks through it step by step.
flowchart TD
A[No treadmill available] --> B{Graded test possible?}
B -->|Bike + staff| C[BCBT / submax bike → HRt prescription]
B -->|Field + trained staff| D[mSRT or structured field exertion]
B -->|Neither| E{Reliable HR monitor?}
E -->|Yes| F[Age-% band 50–60% start + symptom cap]
E -->|No| G[Symptom cap only ≤2/10]
C --> H[24h rule before advance]
D --> H
F --> H
G --> H
H --> I{BCTT later available?}
I -->|Yes| J[Re-anchor to 80% HRt]
I -->|No| K[Continue band + symptoms]
Vignette
A 16-year-old midfielder has headache and fog 35 days after a collision. Your school has no treadmill. The nearest concussion clinic is three weeks out. Parents can supervise 20-minute walks after school. The athlete has no red flags; vestibular symptoms are mild and triggered mainly by rapid head turns in crowded hallways.
This patient matches Setting A. Deferring all exercise until BCTT becomes available would be a mistake—the literature supports structured sub-symptom activity in prolonged symptoms PMID: 33147117 PMID: 29058559. The better move is to pick the highest-precision path available now, not the path with the most PubMed citations.
Work through the plan in order:
Graded test feasible this week? Bike → BCBT or submax bike 31488375. Gym only → mSRT only if staff trained; not unsupervised shuttle runs 35894897. Neither → formula or symptom path.
No test: Start conservative—50–60% age-predicted HRmax or symptom cap ≤2/10 32079897 30742254. Prefer chest strap over wrist optical if available.
Progression: 24 hours without symptom escalation before advancing (Berlin/CISG-style community staging) unless a later HRt enables Buffalo-style titration.
Stop rule: Symptoms ≥2 points above session baseline → stop; do not push to hit a percentage target.
Environmental note: Most validation data come from indoor, temperate, supervised settings. High altitude, cold, or ice surfaces change perceived exertion without published PPCS correction factors PMID: 30742254. Treat any HR target as an upper bound; weight symptoms more heavily.
What to tell the family: “After school, walk fast enough to finish a sentence without gasping—about twenty minutes if the schedule allows. If headache or fog jumps more than two points from when you started, stop and text us. This week we’re calibrating what your brain will tolerate, not training for a fitness test.” If they have a chest strap, add: “Stay near the low end of the number we wrote; it’s a ceiling, not a target.”
When to escalate to measured testing: Symptoms plateau beyond two weeks on a no-BCTT path; vestibular symptoms dominate and treadmill provocation is a concern (consider BCBT referral); or return-to-contact sport is approaching and the team wants a documented threshold. None of those scenarios invalidates the home path you started—they define when precision becomes worth the access cost.
5. SOP checklist and educational tool layer
One-page SOP (no-BCTT community default)
Synthesizes McIntyre, Dobney, Jaganathan, and symptom-limited stop rules for education only PMID: 32079897 PMID: 29058559 PMID: 36940683 PMID: 30742254.
| Clinician | Parent | Adolescent |
|---|---|---|
| □ Red flags screened; no BCTT if acutely unstable | □ Know emergency signs: repeated vomiting, worst headache, slurred speech | □ Rate headache/dizziness/nausea 0–10 morning and after exercise |
| □ Pick path from Figure 4 (bike / field / formula / symptom) | □ 20 min supervised aerobic if cleared; walk or easy bike | □ Stop if symptoms +2/10 vs session start |
| □ Document which anchor used (% band, RPE, or cap only) | □ Log date, duration, peak symptoms—not only “felt fine” | □ Able to speak full sentences without gasping |
| □ If HR monitor used: note device type (chest vs wrist) | □ Do not advance duration and intensity same day | □ Schoolwork in blocks; rest eyes if screen triggers fog |
| □ Advance after ≥24 h without escalation | □ Escalate to clinician if 2 bad days in a row | □ No contact sport without written clearance |
| □ Re-refer for BCTT/BCBT if plateau >2 weeks | □ Photo clearance letter for coach/school | □ Step back one level if symptoms return next morning |
PPCSexRx — illustration only (Figure 5)
Important
Educational use only. GRADE: LOW certainty. Outputs from the published CRAN package PPCSexRx. Not clinical advice or a mandated protocol.
The package PPCSexRx exposes a transparent fallback: with hrst, prescription uses BCTT-guided logic; without it, an age-predicted band. This piece uses only screen_ppcs() and prescribe_ppcs().
library(PPCSexRx)
screen_ppcs(age = 16, days_post_injury = 35)
prescribe_ppcs(age = 16, days_post_injury = 35)
prescribe_ppcs(age = 17, days_post_injury = 40, hrst = 160)Scenario A — No BCTT (age 16, day 35)
Target HR133 bpm
Duration20 min/session
Frequency5 sessions/week
MethodAge-predicted 60–70% HRmax
HRmax basis220 − age = 204 → 133 ≈ 65% mid-band
Scenario B — HRt = 160 bpm (age 17, day 40)
Target HR128 bpm
Duration20 min/session
Frequency5 sessions/week
Method80% of symptom threshold HR
Rather than debating which number is “correct,” the pair shows what changes when HRt enters the model. Scenario A encodes the package’s default 220−age fallback when testing is unavailable—the same denominator most published %HR bands assume, not the youth-adjusted 208−0.7×age formula discussed in §3.2 (which would land nearer 127 bpm at 65% for age 16). Scenario B restores Buffalo logic once a threshold exists—even if that test happened at a referral center weeks into symptoms.
Parents and athletes still need symptom caps from the SOP table. Package output does not replace observation. Jaganathan’s HR + RPE pairing remains relevant PMID: 36940683. Session logging across visits—useful when the prescription anchor changes after a late BCTT referral—is documented in the package vignette.
Do not read the package as adjudicating between 50%, 60%, or 65% bands. It implements one published fallback encoding. Your clinical judgment—and the setting matrix in Figure 3—still determines whether a formula, RPE, or symptom-only path is appropriate before any code runs.
6. Limitations
Validation gap: Fallback percentages are assembled from reviews and heterogeneous trials—not one head-to-head RCT of “BCTT vs 60% age-predicted HR” in adolescent PPCS PMID: 32079897.
Formula uncertainty: 220−age dominates the literature; youth-adjusted formulae are rarely specified in PPCS trials.
Setting transfer: Bike and field substitutes are validated in specific cohorts; mSRT comparisons included recovered-history controls PMID: 35894897.
Device error: Consumer wearables may mis-estimate intensity versus chest ECG in BCTT studies PMID: 30742254.
Tool layer: PPCSexRx illustrates encoding of published fallback logic; it is not regulated medical device software.
Adherence: Trial supervision often exceeds what home programs achieve; this SOP does not solve unsupervised execution PMID: 27120294.
Scope: Fallback-path synthesis for education—not a substitute for local return-to-play law or individualized clearance.
What these limitations mean in practice
The most significant limitation for community settings is the gap between trial conditions and family execution. That gap isn’t a reason to withhold exercise prescription when BCTT is inaccessible—it’s a reason to document the path chosen, calibrate expectations, and build the SOP around what parents can sustain instead of assuming lab conditions apply by default.
When symptom-threshold treadmill testing is unavailable, the literature offers multiple defensible paths rather than a single defensible number. Bike tests, field tests, overlapping age-percentage bands, and symptom caps each trade precision for reach. Castellana et al. suggest measured Buffalo prescriptions and “light effort” age bands may land in a similar zone for adolescents, but that observation bridges two literatures—it does not merge them into one protocol PMID: 38980666.
Series: Foundation Stack · methods · no-BCTT fallback paths